

atoq
-
Posts
55 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Posts posted by atoq
-
-
6 hours ago, tom webster said:
6) Vancouver - they've been out of the playoffs since 2014/2015 I believe
Strange point to make about Vancouver in a post about how we shouldn't focus too much on the distant past with the Sabres. More relevant with Vancouver is that they are one of the top teams in the league this year, but that doesn't back up the "other organizations aren't passing us by" conclusion you're straining for.
-
11 hours ago, Pimlach said:
I assume this is a joke? Kaleta is no coach.
Matt Ellis as GM and I just might burn my 1970 vintage Sabres Jersey.
9 hours ago, That Aud Smell said:I took @atoq's suggestions as satirical. (Or am I now missing your joke?)
Apologies for making wild exaggerations to suggest someone could be promoted from failed Sabres assistant coach to Sabres GM without first managing the Harborcenter.
-
 5
5
-
 2
2
-
-
My prediction:
Assistant coaches: Nathan Paetsch and Patrick Kaleta
Matt Ellis promoted to GM.
Kevyn Adams promoted to President and extended.
We want people that can't go anywhere else, I mean, that want to be here. Hire from within to keep developing the organizational culture. Outside voices concerned with winning will only create conflict in the locker room.
-
 1
1
-
2
-
-
20 hours ago, Weave said:
This is ***** stupid. Its a beer league. Everyone is there for recreation and exercise. Everyone has a real job to get to the next day. It’s absolutely ridiculous to expect someone in that situation to have the means, personality, or will to come to someone’s aid here. It’s a ***** beer league.
And yeah, some white knight should have come to defend her honor. Now there is some real progress. LMAO
She came into a situation where she expected to be treated as equal. Was plastered in a league that certainly regulated contact, as evidenced by the penalty handed out. And then taunted afterwards. And she’s the one who handled it poorly. *eyeroll*
I totally agree with this.
Some absolutely terrible takes in this thread. To those posters, you aren't coming across as bravely un-PC, you just look like idiots.
-
 1
1
-
-
You all need to be more patient. It's only fair to give Matt Ellis a few more years to learn how to coach the power play.
-
2
-
-
So tired of this loser team.
-
 2
2
-
-
12 minutes ago, Pimlach said:
Highways and interstates ruined the look of the waterfront. They actually made it easier to get downtown but the location of some of them is just wrong aesthetically.
They actually made it easier to leave downtown.
-
1
-
-
21 hours ago, Pimlach said:
I would call the Metro rail a failure since it killed a portion of downtown just to build it.
The highways were the failure that killed much larger portions of downtown.
-
2
-
-
21 minutes ago, thewookie1 said:
There wasn't any this offseason that actually went to UFA
This is the worst argument. Goaltending has been a problem since KA was hired years ago in 2020, and he's only let the position get weaker since then.
-
3
-
-
Besides goaltending, my biggest (yet pettiest) complaint is the "players that want to be here" slogan, which is such a cop-out coming from the person whose literal job it is to convince the right players they should want to be in buffalo, either through financial offerings or by selling the culture/region/future of the team.
Obviously you can't convince everyone, but can we stop repeating this as an organizational motto, especially now that the Eichel-era transition is over? What does this even mean going forward?
-
1
-
 1
1
-
-
3 hours ago, Eleven said:
Seriously, he's had three seasons and nearly four off-seasons to straighten out the goaltending situation. That's his job. Other GMs seem to have managed. If Levi doesn't work out, Adams has to go.
I agree with this take. He's been neglecting the position since he started the job 3 years ago with Ullmark and vision-impaired Hutton on the roster. Not only has he not strengthened the position in the short-term, he let the best option we had walk for absolutely nothing, after the club spent years developing the player (within the division no less) That's just poor asset management, whatever you think about Ullmark or his Vezina. Get the player locked up or find another solution.
I'm excited about Levi's future with the club (almost more than any other prospect), and hope he defies past trends with rookie goalies, but this position is still the biggest doubt going into the season.
Also, the exaggerated topics obviously don't represent what most people think who are critical of recent goaltending decisions. A GM can make good moves, like Adams certainly has, but still neglect key aspects that limit the overall success of the club. Darcy, Murray and Botteril all made some good moves, but made some serious mistakes in specific areas too (playoff toughness, culture/character, finding a good coach, respectively).
-
1
-
1
-
-
23 hours ago, Mustache of God said:
"Why hire a designer when our daughter can do it better?"
A management philosophy that apparently extends to "Why hire a GM when the yes man at the arena can do it better?"
-
1
-
-
23 hours ago, That Aud Smell said:
This guy has squandered a lot of credibility with me since I started following him as a counter-weight to MSM coverage of the pandemic, but this Tweet thread seems to have some merit to it.
^
Lol at "squandered", as if the guy gives a sh1t that he's lost credibility with me, which the term "squandered" implies.
I'm confused. I followed the link to learn more and found a story very different that what this twitter pundit describes, in which Sanford Health is trying to distance themselves from an outgoing executive (who has a business background) who made comments downplaying the crisis and need for masks.
Was the story later updated? Did Alex not read the original story? Did Alex have enough accountability to update his take on the story? As is so often the case with internet pundits, it doesn't appear so.
It also seems he misrepresents how the situation in the Dakota's is being represented, at least in the media. I've seen articles pointing out that the Dakota's have among the worst metrics for hospitalization and mortality rates in the country, and that they are having to allow covid positive medical staff continue to work out of necessity. Both of these seem to indicate there is legitimate reason for concern, and that the situation is precarious.
Is Alex's "team apocalypse" take based on people on Twitter reacting/overreacting to measured stories such as the above? If so, who cares?
-
 1
1
-
-
36 minutes ago, LGR4GM said:
According to reports the affidavits of voter fraud in Michigan are actually using election data from Minnesota because the lawyers for Trump mixed up MN v MI as abbreviations.
That expert confused Minnesota and Michigan. He was counting the population of towns in Minnesota, seeing they did not match Michigan towns, and finding fraud.
That's right up there with bringing a convicted sex-offender from Trenton to Philadelphia to pretend to be a PA poll watcher alleging fraud in a press conference in front of a landscaping company.
-
2
-
-
1 hour ago, nfreeman said:
Well, Sweden has a much lower per capita Covid death rate than Belgium, Spain, France, Italy and the UK, both cumulatively and in the last 14 days.
https://www.statista.com/statistics/1111779/coronavirus-death-rate-europe-by-country/
https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea
So, regardless of how sure one is in one's position, there is plenty of data to support a different view.
I'll also note that I wasn't even advocating for the Swedish approach vs the UK approach -- just pointing out that "the science" isn't "settled."
I agree the science isn't settled and we all have much to learn on the subject.
When reviewing the data, its also important to consider the many factors that impact virus transmission and mortality rates from country to country outside of government policies on lockdowns, including societal factors like population density, health indicators, age distribution, health care system capacity, availability of health insurance, faith in public institutions, and local customs for personal space.
Most of the countries you mentioned that Sweden compares favorably too are in continental Europe. When compared to other Nordic countries, Sweden doesn't look so good anymore.
-
2 hours ago, nfreeman said:
whether approaches like Sweden's are better than approaches like the UK's, and other important issues relating to handling the virus.
The "Swedish model" has been brought up several times in this thread, as though its a strategy that could be implemented in the US. Its important to note the incredible pre-COVID societal differences between the two countries. Here is the ambassador from Sweden explaining some of those differences:
QuoteKarin Ulrika Olofsdotter, the Swedish ambassador in Washington, stressed that widespread trust in the country’s public agencies meant that most Swedes would voluntarily heed social distancing guidelines. Sweden’s robust social safety net and enhanced paid sick leave, she argued, would help ensure more Swedes would stay home if they felt symptoms or feared contracting the virus at their workplaces.
It's also important to note that Sweden has universal public health care (mostly government funded), meaning there aren't ~28 million people without health insurance like in the United States.
@nfreeman Are you advocating for universal health care and enhanced paid sick leave, following the Swedish model? 😃
Over the summer, we were told that Sweden wouldn't face a harsh second wave in the fall due to acquired immunity.
QuoteAnders Tegnell, Sweden’s state epidemiologist...predicted that Sweden would have accrued a higher level of immunity than its neighbors and that the impact of a second wave would “probably be quite low.”
Let's check in on how Sweden has been doing recently with COVID-19. https://www.ft.com/content/1e0ac31d-5abf-4a18-ab3e-eec9744a4d31
Quote“Four days ago [Sweden] had eight times higher cases per capita than Finland and three and a half times more than Norway. They were supposed to have it worse off than us in the autumn because we were going to have immunity.”
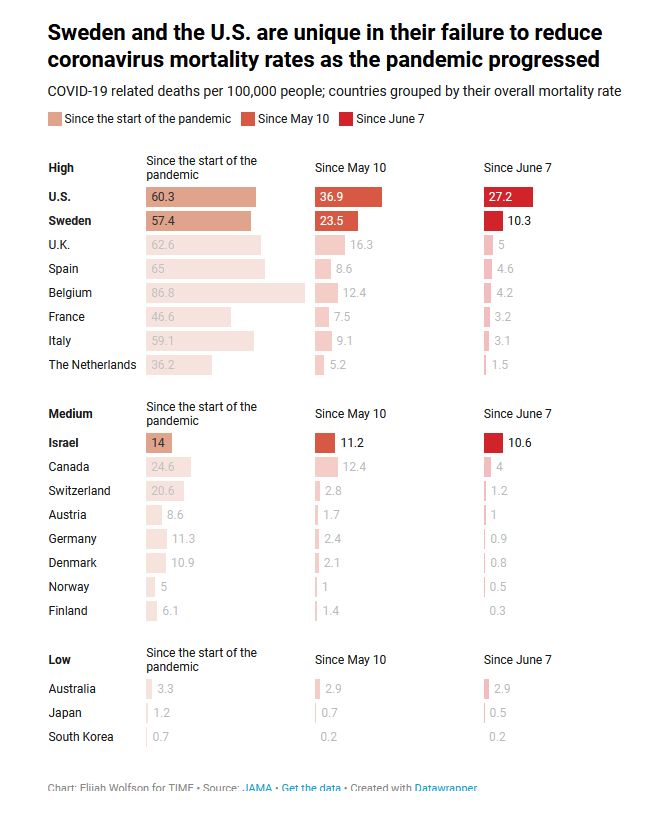
Sweden has also maintained high COVID-19 mortality rates as the pandemic has progressed. .

So people are still getting sick and dying from COVID-19 in Sweden. Following @nfreeman's theory, these losses should be offset by the economic advantages from avoiding lock downs, thereby mitigating cascading negative impacts of job loss and economic hardship.
Sweden's GDP slumped 8.6% in Q2, more sharply than its neighbors despite its no-lockdown policy
https://www.businessinsider.com/coronavirus-sweden-gdp-falls-8pc-in-q2-worse-nordic-neighbors-2020-8
Given all of the above, it seems likely that Sweden will be changing their policies towards COVID-19 in the near future. In fact they've already started this by limiting gathering sizes. It's hard to believe that people still advocate for the "Swedish model" even though recent evidence indicates it isn't working and the baseline social context was so different that this model wouldn't have been replicable in a country like the United States.
-
1
-
3
-
-
4 minutes ago, atoq said:
The correct argument is if this is an election is being rightfully disputed with legitimate evidence (it's not) or if it's being disputed only by a serial-liar and his subordinates who are utilizing wild conspiracy theories, obviously futile legal cases, and pressuring local election committees to throw out votes they don't like in order to subvert our democratic process (it is).
I forgot another way they are attempting to subvert the democratic process: leaning on partisan state legislators to completely ignore the election results in swing states https://www.reuters.com/article/us-usa-election-trump-strategy/trumps-election-power-play-persuade-republican-legislators-to-do-what-u-s-voters-did-not-idUSKBN27Z30G?il=0
-
53 minutes ago, LTS said:
The argument has continued to be, it's disputed (it is) and it's not over (it's not).
The correct argument is if this is an election is being rightfully disputed with legitimate evidence (it's not) or if it's being disputed only by a serial-liar and his subordinates who are utilizing wild conspiracy theories, obviously futile legal cases, and pressuring local election committees to throw out votes they don't like in order to subvert our democratic process (it is).
-
1
-
-
On 10/6/2020 at 8:48 PM, SwampD said:On 10/6/2020 at 6:27 PM, nfreeman said:
9th bolded -- again, this isn't presented as a scientific study. Your (and, to be fair, others') insistence on criticizing it as such is like criticizing an apple for not being an orange, and likely derives from, ironically enough, your cognitive assumptions about what is best for society.
No offense, but seems a bit disingenuous.
The first line of the webpage, "As infectious disease epidemiologists and public health scientists,…" (FTR, wtf is a public health scientist?)
It is absolutely disingenuous. Besides the good points made by @SwampD about the the webpage, let's look to how @nfreeman himself how described the declaration:
On 10/6/2020 at 10:52 AM, nfreeman said:I think the main takeaway from the declaration is that these epidemiologists/HC professionals believe, as a scientific matter, that a broad reopening will have substantially fewer destructive consequences than a broad lockdown.
He claimed this was a scientific take. When it was pointed out there is little to no science in the article, he resorted to name-calling and personal attacks.
@nfreeman you are right, I am a child. And in my first year of middle school I learned that if you want to make a scientific argument, you should provide some data and citations. If you take away the high profile university titles and the number of 'public health scientists', there is no science provided nor productive ideas proposed. It's of course possible that the premise of the declaration is correct or partially correct, but these kinds of decisions should be data-driven because this is matter of life and death for a significant number of people, which was really my point in responding.
Let's look at another recent general non-technical statement by the scientific community, so that we can compare how information is presented: https://www.nejm.org/doi/full/10.1056/NEJMe2029812
This article helps compare global COVID impacts by providing some statistics (with respected sources) like the following:
QuoteAccording to the Johns Hopkins Center for Systems Science and Engineering,1 the United States leads the world in Covid-19 cases and in deaths due to the disease, far exceeding the numbers in much larger countries, such as China. The death rate in this country is more than double that of Canada, exceeds that of Japan, a country with a vulnerable and elderly population, by a factor of almost 50, and even dwarfs the rates in lower-middle-income countries, such as Vietnam, by a factor of almost 2000.
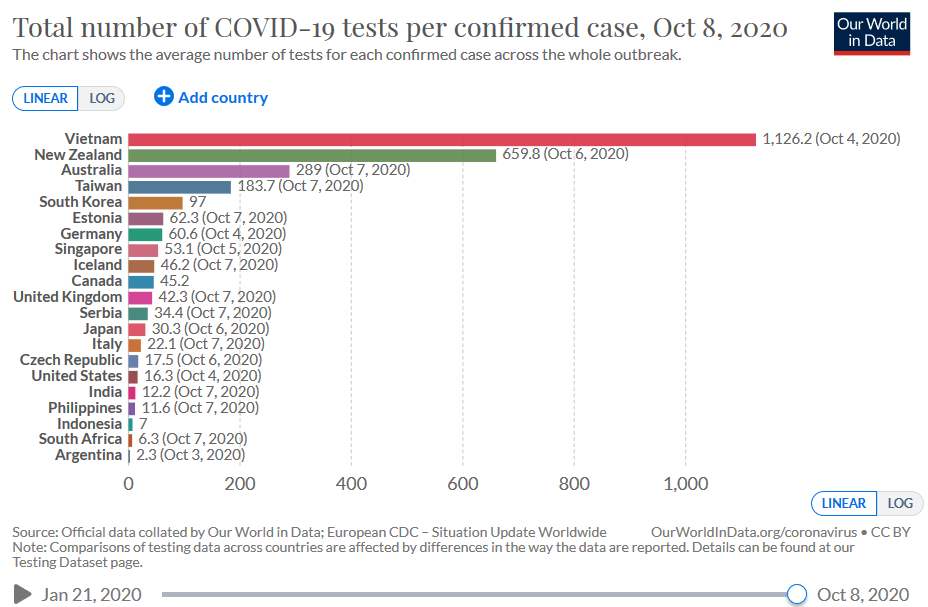
There is also information on how various countries have adapted testing programs, which has proven to be an effective strategy to help reopen economies.
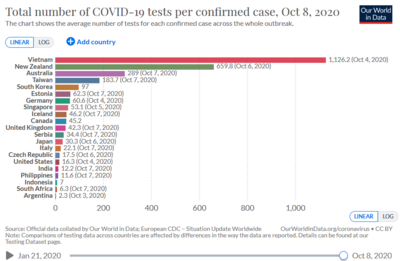
QuoteWhile the absolute numbers of tests have increased substantially [in the US], the more useful metric is the number of tests performed per infected person, a rate that puts us far down the international list, below such places as Kazakhstan, Zimbabwe, and Ethiopia, countries that cannot boast the biomedical infrastructure or the manufacturing capacity that we have.2
There is also a graph provided at the citation link:
As for @nfreeman saying I'm projecting my own cognitive assumptions about what is best for society, at no point have I made the argument that strict lock downs are absolutely necessary. I'm usually only drawn out from lurking when I see really bad science takes that I feel compelled to refute with hopes of an actual ensuing conversation.
Other parts of the world have enacted various strategies that helped dramatically reduce initial COVID infection numbers, followed by careful reopening strategies (a process made easier by more initial control of the virus) that have kept COVID rates substantially lower that in the US. However, I don't think there is currently any political will or capacity to do this in the US, as demonstrated by nearly every step taken in the pandemic response over the past 10 months (see NEJM link above). Even worse, the pandemic has now become another battle in the dumb American Culture Wars (intentionally so, by those who seek to mitigate criticism), where even non-invasive measures that can help vulnerable members of society are perceived as controversial. The shoddy science that surfaces here is part of that.
To the point others have made here, the Great Barrington Declaration is obviously focused on whether or not there should be state-mandated lockdown protocols, in their words "concerns about...impacts of the prevailing COVID-19 policies" (in the title), which makes it a discussion about 'Government responses to COVID', and therefore shouldn't be allowed within this thread. People on this board have been complaining about uneven moderation because mostly political arguments barely obscured behind shoddy science (like Taro's HCQ study and the nfreeman's GBD), have been allowed and even shared by moderators. Yet, reflection or criticism of how governments have handled COVID isn't allowed, even though the options we have today for reopening the economy are directly related to how well the crisis was managed over the past months. Also, if economic concerns are primary, there are a wide range of fiscal policies that can be enacted to help individuals and businesses deal with economic hardships without putting many people's health at risk. This is another entirely underwhelming response that probably can't be mentioned here.
-
6
-
-
1 hour ago, nfreeman said:
First bolded -- do you not think economic activity -- i.e. millions of job losses -- affects public health outcomes?
Second bolded -- no -- they say this, which I also quoted upthread:
Please read more carefully. I repeated the part you quoted about the potential health results. Do you receive vaccinations or cancer screenings at restaurants, museums, concerts, sporting events, etc? There are lots of safe options for outdoor exercise to maintain cardiovascular health, leaving 'deteriorating mental health'. I acknowledged the link between unemployment and deteriorating mental health in bold #2 (perhaps not clearly enough), but the authors provide no evidence or analysis about and whether or not people will be more sad if they lose their job, or if the society lets the virus goes unchecked a lot of people die, including friends and family.
Nor do they make a compelling case for how things can be reopened without unchecked spreading of the virus. Let's check their suggestions.
QuoteAdopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent PCR testing of other staff and all visitors. Staff rotation should be minimized. Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
As discussed, entirely staffing nursing homes with people with acquired immunity is entirely unrealistic given training and overall demands needed to conduct this type of work. It's really hard work and requires training, experience and a certain temperament. That and grocery delivery are the only specific suggestions from this declaration. Otherwise they say its possible to do and well within the scope of their profession. I get this is meant to be a general statement and not a detailed plan, but do you really find this a compelling argument, when they offer no data or specific plans? It seems strange to me this supposed broad coalition of experts can't suggest anything else, and had to resort to "We can totally do this" when the reality of the situation has shown otherwise, given the common dynamic of one superspreader can infect many people.
The highest levels of Western leadership can’t even adhere to suggested bio security rules in their inner circles. Why does the “Great Barrington Declaration,” depend on the fanciful thinking that society at large can functionally implement these safeguards?
1 hour ago, nfreeman said:Third bolded -- I don't see any claim of a consensus anywhere in their statement.
This sentiment is implied in the how the authors (and you and others reposting online) have stressed the prestigious academic institutions involved and the overall number of doctors that have signed on, regardless of their actual expertise in this field.
1 hour ago, nfreeman said:Fourth bolded -- the declaration doesn't claim to be a cost-benefit study that is submitted for peer review.
They are certainly making cost-benefit conclusions that could have serious implications on public health, yet they provide no statistics, citations or evidence to support those conclusions, which is inherently dangerous. The following is literally the only statistic in the entire piece (age stratified mortality):
QuoteWe know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young.
The stat is mentioned tangentially while contrasting the two extreme age groups and ignoring all of the age ranges in between to whom the risk is considerably higher than the flu. A single statistic, poorly explained or even misrepresented, is inexcusably sloppy. The role of data driven decision making is not discussed once, despite the number of biostatisticians and epidemiologists that have signed this document. Of course it doesn't claim to be submitted for peer-review, because the authors would undoubtedly know given their professions that any scientific conclusions provided without any evidence would be immediately dismissed. My point is this declaration doesn't pass any scientific muster. These are people who are using their positions and credibility to bend science to what they believe is best for society.
1 hour ago, nfreeman said:Sixth bolded -- what is your expertise in this area? Is it comparable to that of the authors?
Nice try, making this about my expertise. I engage with the scientific community enough to know that the scientific method is based on observation, empiricism, rigor, and skepticism of cognitive assumptions. This declaration doesn't involve any of these things. I won't ask for your credentials.
-
1
-
1
-
-
46 minutes ago, nfreeman said:
I think the main takeaway from the declaration is that these epidemiologists/HC professionals believe, as a scientific matter, that a broad reopening will have substantially fewer destructive consequences than a broad lockdown.
This piece begins with an attempt to make a scientific argument about public health (cancer screenings, vaccinations, etc.) and concern for the underprivileged, and then finishes by advocating for a broad reopening of sports, schools and cultural institutions, which seem much more related to economic activity than public health outcomes, and therefore not a 'scientific matter'. The only link between what they propose to reopen and public health is the vague mention of 'mental health deterioration', which also likely applies to the friends and families of the 210,000 people who have died in the US alone.
Some more issues with this site: They are trying to convey their perspective as the consensus view among epidemiologists, and that is certainly not the case. Many of the public health professionals that signed onto this declaration are not epidemiologists. Some of the signatories have published highly flawed statistical models https://statmodeling.stat.columbia.edu/2020/04/19/fatal-flaws-in-stanford-study-of-coronavirus-prevalence/ Furthermore the authors provide no information on the basis of their argument, whether it be citations to peer-reviewed scientific papers or details on the cost-benefit analysis utilized to arrive at their conclusion, instead hoping the reader will take their word given their positions of authority. They likely issued an open-letter knowing this wouldn't pass peer review. There are a ton of variables that would influence a cost-benefit study like this, including what timeline did they consider for a potential vaccine? Some of their suggestions for reopening are nonsensical. How feasible does it seem to entirely staff nursing homes with people who have acquired immunity?
In my opinion, this website doesn't hold up to scientific or general critical review and is only intended to provide fodder for politicians to say "See, the scientists said we can reopen" and for politically motivated contrarians to champion on internet message boards.
I also totally agree with Weave's take that separating the vulnerable from the non-vulnerable in our society would be almost impossible. The US government has been unable to provide consistent messaging on fundamental aspects of virus control (does mask wearing work?, can the virus can be transmitted through the air? etc.). The highest level decision makers in the US are unable to abide by basic mask wearing, testing, and self-isolation protocols to protect small, affluent and isolated groups of people, yet some think its realistic be able to carefully separate out the millions of vulnerable people in our society?
-
1
-
1
-
-
4 hours ago, Wyldnwoody44 said:
I can literally fly to south America with no safeguards in place, no quarantine, no testing, etc.
This is literally not true for the majority of South American countries. You mentioned Brasil, which is an outlier in their COVID response strategies, and the effectiveness of their strategies is demonstrated in their COVID case count number, the number of people who have died there, and how Brasilians have spread COVID into border regions of neighboring countries.
13 minutes ago, Wyldnwoody44 said:I'm currently not able to go to other countries to help other people who are dying of disease(s) that they have 0% chance of preventing because of a disease here that mainly wouldn't be as bad if we weren't selfish, fat, pieces of American embodiment.
Please look into how COVID is impacting communities in developing countries. Health facilities have been close to collapse for months in many countries. Indigenous communities in South America have been devastated by the virus, not because they are selfish and fat, but because they have genetic deposition to diabetes.
Look, I agree with your anger about indifference for people dying from other diseases in the past. We don't fix that as a society with continued indifference to people dying from diseases.
22 hours ago, nfreeman said:Continental Europe has more than double the US population, and they have largely re-opened to a greater degree than we have
How does the COVID case count and # of deaths in continental Europe compare to the US? Is it more or less than the US? (Keeping in mind they have double the US population, of course) What did they do differently than the US between February and August?
19 hours ago, PASabreFan said:I scratch my head at how smart people can miss the obvious culprit in our economic and societal woes: the virus. Not the mitigation efforts. We get back to normal by cutting down the virus to very low levels, which is achievable, because other countries have done it. Then, and only then, can the economy fully come back.
This is exactly right. Tenet didn't bomb because theaters were closed, it bombed because people were afraid to go to the theater because of the virus. Now those theaters lost money opening the doors and paying staff for only few people to show up. A long lingering virus will prevent people from wanting to go to bars, restaurants, etc. If those institutions are trying to open, paying staff, etc and no one is going, its an even worse scenario.
Something like a short term rent-relief program on top of the minimal economic packages that were passed could have helped businesses deal with a strict lockdown for a matter of months so that we would be better positioned to reopen the economy for the coming year, like many other nations have done. Now we're stuck in limbo.
The long-term economic devastation argument is valid for sure, unfortunately the same crowd was making this argument in March and April, likely in-part related to the politicization of the virus, which prevented the US from ever getting control of the virus in the first place. If the US had done that, it would be easier to reopen like other places are now.
14 minutes ago, LTS said:Except they can go to out of state tournaments as long as that state is not on the list.
It's almost like some level of coordination above the states was needed to mitigate the inconsistent implementation of known-effective policies that have led to some areas being much safer than others.
Also want to add, besides possible death from COVID, the long-term health implications of the virus are not fully understood, with indications it can have affect someone's heart, brain and lungs. Another reason for caution.
-
On 8/5/2020 at 9:45 PM, Taro T said:
You produce a 5 paragraph novella because you didn't see the word "about" in a sentence you bolded, but then say others don't read things carefully.
You ask people to read 60+ articles and roll your eyes at 5 paragraphs. I did misquote, having originally intended to quote more and respond point by point, but instead responding more generally to the series of posts the followed. Oh well, nobody is perfect, I made careless mistakes in my post and you look for medical advice on a political sub-forum of a NFL message board. We're all doing our best.
On 8/5/2020 at 9:45 PM, Taro T said:And presumably upon reflection, as the comment was added much later, you seem to agree that the point of getting people access to papers so they can read for themselves is important.
3 minutes later. Nice try.
On 8/5/2020 at 9:45 PM, Taro T said:And that is all the original post on this subject was doing; proving people a source to access studies directly without having to rely on somebody else's interpretation of those studies.
I think we can all get behind more quality science being made available to the public. However, in this case there was curation and interpretation of those studies, as well as misleading design elements on the page itself. I think 100% agree that it's a good thing that people read more science papers, but its also fair to say that trained experts are much more equipped to review, interpret and make decisions on this type of work. Let's be honest, neither you nor are I nearly as informed as we like to claim we are in internet message board arguments.
On 8/5/2020 at 9:45 PM, Taro T said:Please show us anywhere where yours truly has touted not social distancing, ignoring proper hygiene, or not researching other potential treatments & vaccines.
Please show me anywhere where I accused you of touting not social distancing, ignoring proper hygiene. As I had discussed in the previous paragraph, there is an undeniable segment of the population whose perspective on HCQ is influenced by the idea that the severity of the virus has been exaggerated, lock downs were/are unnecessary (and politically motivated), and that known medicines that work are being suppressed. People with these views are more likely to not wear masks and ignore social distancing protocols. Those viewpoints are widely expressed where you found the link, just one step away from this message board. I intentionally tried not to reference you specifically in this group (and certainly not shrader) to give you the benefit of the doubt that although you frequent those site and often share their content, you don't buy into the conspiracy theories.
Let's look at a case study of a public figure, Herman Cain, who touted HCQ treatment from March-June, later attended a large public event in late June against recommended social distancing protocols while also not wearing a mask (even though he touted mask wearing on his site), to later catch and die from COVID. He obviously understood the importance of masks and social distancing yet irrationally disregarded all of that advice. Obviously we can't say for certain if he took those risks because he thought he could rely on HCQ, but HCQ was certainly in the equation given how outspoken Cain was on the topic.
On 8/5/2020 at 9:45 PM, Taro T said:Premature celebration of an unproven treatment IS a bad thing.
So then you agree that high profile government officials promoting the use of an unproven treatment is irresponsible? Especially given that it led to people taking a non-FDA approved medicine shown to potentially have side-effects, as well as causing a rush for those drugs thus limiting availability for those who may need the medicines for other conditions?
On 8/5/2020 at 9:45 PM, Taro T said:Also, not sure how you concluded that researchers worldwide studying whether HCQ based treatment regimens were viable was altering public policy appreciably causing the virus to spread. Don't agree with that take, but not a big deal.
This isn't what I was saying, and I think you're being deliberately obtuse here. The pandemic response is as much as a social experiment as one of policy. We need both common-sense public policy that researches potential treatment and vaccines while at the same time enacting communication strategies that promote social behaviors that will keep the virus from spreading. I think we need both carrot-and-stick aspects to policy, in which certain standards are established with regards to use of masks, social distancing, testing and contact-tracing (stick) but perhaps even more more importantly, that these policies are bound together by cohesive public messaging that encourages mutually respectful behaviors that help slow the virus from spreading (carrot). I think it would be difficult to argue that either of these has happened in a country with the highest COVID case count and number of deaths in the world. I refer to HCQ as a distraction because policy and cohesive communications efforts have obviously proven insufficient so far, yet there has been a tremendous public focus on HCQ due to certain individuals, which has only created unnecessary debate, division and confusion.
Is there a good reason for publicly promoting unproven HCQ as a solution while publicly downplaying proven solutions like extensive testing and contact tracing (and even masks up until the past weeks)? Is this dichotomy due to concern for public health outcomes, or because there hasn't been enough tests available but lots of HCQ available? Do you think it is a coincidence that many of the countries most badly affected by COVID (US, Brazil, Mexico, India, Venezuela) are all promoting unproven medications?
Shrader very well may be right that a certain segment of the population would ignore masks and social distancing recommendations anyway, for the reasons he listed. I see the HCQ conversation as just a small part of a larger discourse that attempts to minimize the severity of the virus, further emboldening those people to ignore public health advice.
I assume the scientists are continually doing their jobs looking for treatment and cures, the main failure I see has been with communication and community building strategies to foster the public cohesion needed to stop a pandemic. Undue and premature focus on HCQ has only worsened this. Is waiting for FDA approval considered a controversial stance in the US these days?
-
On 8/3/2020 at 11:37 AM, Taro T said:
Um, there was no editorializing about the website & it provides links to many studies directly (including studies that lean positive, negative, & inconclusive) and includes whether they were peer reviewed or not. Seems that having direct access to studies that often can be locked behind paywalls would be a good thing.
If you don't want to check out the studies, that absolutely is your prerogative. But sending the OP into a politics thread that will have limited views seems to be counterproductive.
To the bold: Yes there was. The website selectively chooses studies, ignores the quality of the evidence, misrepresents the conclusions of studies, and fails to consider how studies compare to each other in terms of cases studies. The graphic at the top of the page is also complete BS and entirely misleading for reasons mentioned earlier, mainly leaving out Brazil, but also in it's general design and inclusion of debatable labels that reveal the agenda behind the site instead of letting the data speak for itself. Design is important, especially on the internet, and the misleading graph and tagline in bold are clearly given center stage at the top of the site. The graph has been widely shared on social media as this website has been disseminated (more on that later). That is the primary messaging of this website.
I agree with you that in an ideal world everyone would do their homework and read through the studies (or at least summaries) to draw their own informed conclusions. However that doesn't change the fundamentally flawed nature of this website. This website clearly makes it's argument at the top of the page, and it is asking a lot of people to click through hundreds of links and to read scientific articles about something that the creators of the website essentially presented as fact. That's expecting an awful lot from the general public, especially when you yourself have seemingly put little critical thought into the validity of the website as an independent data aggregation source.
I should have explained better my comment about how this website has been disseminated, which I think also ties into @Taro T's point about stereotypes about people hopeful about HCQ. Looking at reddit and twitter, this site is most popular in conspiracy theory communities, where the underlying narrative is that HCQ is being suppressed by the [CENSORED] to implement shut-downs to intentionally damage the economy and prevent [REDACTED] from being [CENSORED]. @Taro T and I have discussed information sources in other threads, so I went to his favorite news source: Two Bills Drive, Politics, Polls and Pundits, and sure enough c19study.com was posted there the day before Taro shared it here. On TBD the site was posted alongside many of the previously mentioned conspiracy theories and the misleading graph was also highlighted. I wonder: how many of those readers took the prerogative to read the actual studies? This HCQ website was initially shared on TBD via The Gateway Pundit, a website that is rated by multiple media review sites as having extreme bias with poor sourcing of credible information and prone to promoting conspiracy theories. So, if we follow the chain, c19study.com is being promoted on unreliable political news sources, picked up and disseminated in online communities where political conspiracy theories flourish (TBD, reddit conspiracy theory) and now being presented as an independent scientific data aggregation resource in a supposedly apolitical thread focused on the public health. When the flaws of the website were pointed out, the OP chided others for not doing their investigative homework in reading through the studies.
Look, I think we are all hopeful that existing and affordable medicines will prove effective at treating COVID. These are difficult times and we are all looking for answers. I didn't meant to stereotype those with interest in HCQ treatments, but given the brief review above it's undeniable that there is a segment of the population have latched onto HCQ for reasons beyond public health concerns, and that for those people, it is often a question of HCQ treatment vs wearing masks, quarantine and social distancing protocols. While I can understand if someone would want to take HCQ in consultation with their doctor, I would also hope that others could understand that others might opt against it, especially in pre-exposure or post-exposure stages, given the general side effects, possible complications, and lack of conclusive scientific evidence of the benefits in relation to COVID outcomes. For this reason and others, it's important that sufficient public health strategies are developed to not have to overly rely on unproven medications until they can be tested and approved by the FDA. Some people are justifiably worried that strategies to protect people's health (or at least public messaging on those strategies) have been overly-focused on unproven medications like HCQ at the expense of planning for solutions that have worked in other countries and in the US in previous months.
Thank you to @Taro T and @shrader for pointing out mine and other's imprecise usage of the word 'miracle cure'. I think my use of the word cure was a bit sarcastic and less in reference to how HCQ treats the virus and more in reference to the socioeconomic context, where many people seem to believe that we can continue on with business-as-usual and deal with letting the virus run rampant by treating it with HCQ or other existing medicines. Given that these treatments are still unproven, the seemingly prudent thing to do would be to try to prevent the virus from running rampant until more testing has been done. Premature celebration and promotion of unproven drugs, alongside the general downplaying of the severity of the virus, has undermined social distancing efforts and lead to more community spread. For this reason, in my opinion, until more evidence exists that COVID can be safely treated with HCQ, this debate is only a distraction from necessary and difficult conversations we need to have as a country on what can be done to protect public health while also protecting American individuals and businesses from impending economic disaster, as well as a distraction from developing realistic education strategies instead of trying to reopen schools, etc given how widespread the virus is in the US.
Edit: I've seen access to scientific papers mentioned in this thread. I think this topic is so vitally important because quality scientific information is so often hidden behind a paywall while misinformation is freely disseminated and promoted. For anyone looking to access academic papers try googling sci hub.
-
4
-
Kevyn and Don, should we really expect more after four years?
in The Aud Club
Posted
Ok, but who signed him to a 1 year deal via arbitration walking him to unrestricted free agency? Either lock up the player or trade him if he isn't in the plan. It's poor asset management. A common argument here is "it's not easy for KA to pick up a good goalie". Yes, because good GMs don't give them away for nothing.
I believe Ullmark felt he needed a personal change. I don't believe for a second that going from a perennial losing team (after one of their worst seasons) to one of the best teams in the league didn't factor into his decision making, especially when the good team shows they want you by offering more money not pinching pennies in arbitration. Not something someone would likely say to the press, and not a compelling personal story a league reporter may choose to focus on.